Over the past few weeks, as the number of reported U.S. deaths from COVID-19 approached 200,000, I have puzzled over why the fewer than 3,000 lives initially lost in the terrorist attacks of September 11, 2001 united our country, but the far higher toll of COVID-19 (at one point over the summer, more than 2,000 were dying each day) has only seemed to divide us. One reason is obvious: after 9/11 we quickly identified a clear villain in Al-Qaeda, while - despite attempts to assign responsibility to the Chinese government for its early inaction - rallying Americans against an unthinking viral enemy is more challenging. Another reason is that President Donald Trump is not President George W. Bush. But there's a third reason, too: everyone I know seems to know someone (or know someone who knows someone) who died in the 9/11 attacks. The victims include one of my high school classmates who was working at the Pentagon and a physician who worked at the hospital where I was a family medicine resident at that time. Statistically, it ought to be 67 times as likely that I would know someone who died from COVID-19, but if I wasn't a doctor, that wouldn't be true. (In my DC practice, several patients were hospitalized for in the spring and summer, and the husband of one of my patients died.)
How can that be? It got me thinking about the spectrum of people who have died from COVID-19 compared to the immediate casualties of 9/11. Although one might assume that workers in the Twin Towers, the Pentagon, and United Airlines Flight 93 would tilt white and upper-class, victims included not only stockbrokers and investment bankers but office assistants, cafeteria workers, maintenance workers, and janitors - people from all walks of life. In comparison, about half of those who died from COVID-19 in the U.S. were residents or employees of nursing homes. Of the remainder, Black, Hispanic, and American Indian / Alaska Native persons are far more likely to have been affected; according to data from the CDC, a member of those groups is 3 times as likely to have been infected, 5 times as likely to have been hospitalized, and up to twice as likely to have died from COVID-19. So if your immediate social circle includes few people over 65 or people of color, there's a reasonable chance that you don't know anyone who's become severely ill or died from the infection.
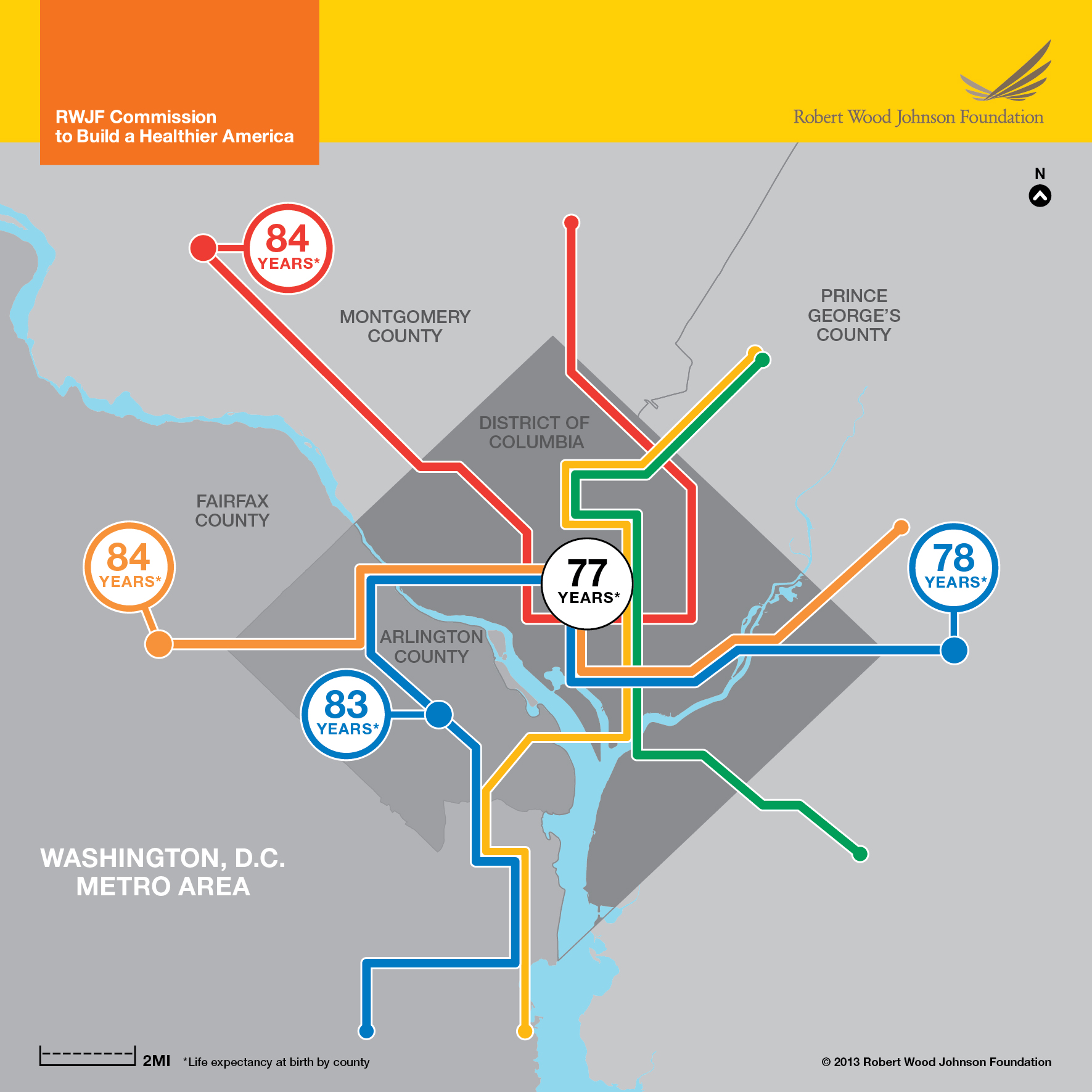
For the past several years, one of my Georgetown colleagues has shown this map in the first lecture of my medical school course "Patients, Populations and Policy." The brightly colored lines trace the paths of Washington, DC Metro lines; the numbers are life expectancy at birth in years. At first glance, the take home point might appear to be that people live longer in the suburbs than in the inner city. But that's not quite right, since life expectancy east of DC, in Maryland's Prince Georges County, is 78 years, nearly the same as life expectancy of someone living near DC's Metro Center, where three of the subway lines come together. What's different about PG County compared to neighboring Montgomery County and Fairfax and Arlington Counties in suburban northern Virginia? PG County is 63% African American, while the corresponding percentages for DC, Montgomery, Fairfax, and Arlington are 47%, 20%, 11%, and 10%.
As stark as the disparity in longevity appears in this map from 2013, it has actually worsened since then. A recent analysis in the scientific journal Nature found that a non-Hispanic White male resident of DC in 2016 had a life expectancy of 86 years, while a non-Hispanic Black male could expect to live to 68. Among female DC residents, the gap was a smaller but still startling 12 years (89 vs. 77). Deconstructing these life expectancy gaps, the researchers found that heart disease, cancer, and homicide accounted for about half of the gap among men, while heart disease, cancer, and unintentional injuries accounted for more than half of the gap among women. Some of the widening gap is no doubt related to gentrification, residential segregation, and migration of higher-income Black persons from DC to PG County (where the COVID-19 death rate has actually been higher than that in DC itself). Disparities in overall health have thus far been closely tied to COVID-19's impact: deaths in the DC's primarily White and Asian populated Wards have been much lower than those in Wards with larger numbers of Black and Hispanic residents.
A note of caution: although age and race inequalities largely explain America's uneven experience of COVID-19 to date, that is no assurance that it will stay that way. HIV/AIDS was a viral disease that only affected urban gay men and intravenous drug users - until it wasn't. Consider Utah, the youngest state in the nation, where 4 out of 5 residents are White, which has largely been spared from COVID-19 compared to older and more diverse states such as California, Florida, and New York. After averaging 300-400 cases per day during late summer, the state's case count has surged above 1000 for each of the past two days, and though much of this increase is occurring in young adults (age 18-39), hospitalizations are starting to rise, too. As far as this virus is concerned, anyone sick enough to require hospitalization is sick enough to die. This health crisis remains as urgent today as it was in early March, and our best tools remain those of public health, not medicine. Just as America united against Al-Qaeda after 9/11, a unified national response to the coronavirus, which has thus far been sorely lacking, is desperately needed.












